Make sure you’re prepared
The most effective management of achondroplasia means anticipating specific complications at every stage of development.
Short stature is a measurable characteristic of achondroplasia, and complications can develop as a result of impaired bone growth. This includes broader health implications such as delayed motor development, chronic otitis media, and sleep disordered breathing in childhood, and spinal stenosis, chronic pain, and mobility issues in adults, just to name a few.

While there is no impact on cognitive functioning, children with achondroplasia are faced with musculoskeletal, otolaryngological, neurological and spinal complications, some of which may require surgery to be corrected.1-3
The most effective management of achondroplasia means anticipating specific complications at every stage of development.
Keep these complications top-of-mind to help give families a perspective of what to watch out for2-9
Affects >50% of people with achondroplasia
Can affect walking and running
Can lead to leg weakness, incontinence, and chronic pain
Can result in loss of mobility
May require physical therapy
Affects up to 70% of children
Crowded teeth and a narrow upper jaw may lead to a crossbite
Limits range of motion
Can lead to high blood pressure or heart disease
Although complications may resolve over time, anticipatory management may help mitigate serious, otherwise unexpected health consequences. Explore the below preparations that could be made to combat the effects of achondroplasia.
Impaired bone growth affects the entire body, and its impact on the size and shape of the foramen magnum can lead to cervicomedullary compression. This can put infants at risk for sudden death, making regular monitoring, management, and timely referrals crucial for this stage.2,3,7,10-16
It is important to keep an eye on complications that can quickly—and quietly—progress.
In addition to the continued risk of sudden death due to cervicomedullary compression, toddlers may experience Achondroplasiadevelopmental delays and other complications that will require familial expectation-setting and potential surgical intervention.2,5,7,11-14,17-20
Throughout their childhood, it’s important to keep an eye out for otolaryngologic, respiratory, and orthopedic issues that have the potential to delay developmental milestones if left untreated. Cognition is not affected in most.2,7,13,19,20-24
At this age, the psychosocial impact of achondroplasia (depression, anxiety, isolation) can begin to impact school performance and social interaction.20,25
Teenage years are a time of great transition for everyone, and while certain medical complications may persist, the functional and emotional implications of living with achondroplasia may become more pronounced. Working with parents, caregivers, and teenagers to address all challenges holistically throughout this time is essential to promoting independence and strong self-esteem.2,5,7,25
Managing both the psychosocial impact and functional challenges of achondroplasia can help in making a smooth transition into adulthood, including higher education pursuits and establishing healthy social networks.
As a person with achondroplasia reaches adulthood, some medical complications may resolve, but others may become more serious and life-threatening. Facilitating a relationship between your patient and the other specialists in their care team is a crucial part of ongoing management. Anticipatory management of this lifelong impact can help mitigate its severity.2,3,7-9,17,26,27
Children with achondroplasia may face both functional and psychosocial challenges, especially as they enter school and transition into puberty. Setting expectations will better equip parents to support their child’s needs.2,18,20
In achondroplasia, complications are not thought to affect cognitive development13,21

Achondroplasia can be overwhelming if foreseeable complications are not properly planned for. It is important to coordinate care with a multidisciplinary team of specialists that proactively manages complications to ensure better patient outcomes.2,4

Primary care providers can help to coordinate a multidisciplinary approach to care
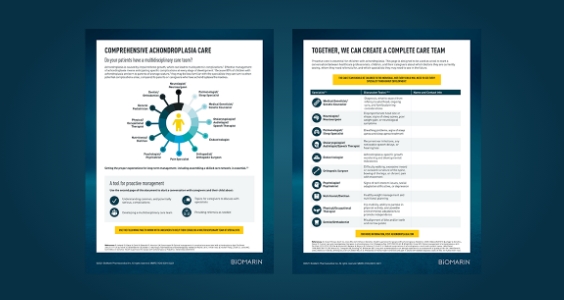
It is important to coordinate care with a multidisciplinary team of specialists that proactively manages complications2,4
